We help you take better care of your feet
At Adelaide Ambulatory Day Surgery, our professionals provide a wide range of services to diagnose and treat a variety of foot conditions. Conditions we help our patients with include conditions such as Corns, ingrown toenails, warts, cysts & soft tissue masses, Morton's neuroma, hallux valgus deformity (bunions) and toe deformities such as hammertoe.
Corns & Calluses
If you find that a corn regrows very quickly and becomes painful despite treatment by your podiatrist then the problem is more than just skin deep. If a corn is back and painful again 4-8 weeks after debridement and your shoes are of adequate width and depth then you need to consider two things:
- It’s about the bone underneath the corn, usually a prominent piece of bone (exostosis)
- It’s about how the toe is aligned – if the toe is rotated or deformed such as in a hammertoe or mallet toe extreme pressure is being generated over an area of the toe during walking
A stubborn corn is not just simply a problem with the skin, but often related to a problem with bone and the rotation and flexibility of the toe itself. Curing the problem will involve minor surgery to address the bone and realign the toe. Unfortunately it is not just a matter of cutting the corn out. It is a myth that corns grow from a root, but a fact that getting to the root of the problem is by cutting the bone and often realigning the toe.
Ingrown Toenails
If you have a recurrent problem with ingrown toenails despite attempts at ‘growing them out’ by your podiatrist, then surgery will often offer a cure. Nails that get infected and do not respond with antibiotics often require a permanent procedure. The most common procedures include the following.
Chemical matrixecotmy
This is a minor surgical procedure, which involves removing the offending piece of nail. A nail splitter is used to remove a small section of nail up to the nail fold. A beaver blade is then used to release the nail underneath the nail fold without having to cut the flesh. This frees the offending nail edge. Once it removed from the nail groove it exposes the nail root from which the nail grows. A chemical (phenol) is then used to burn or cauterise the nail root to prevent the nail from re-growing.
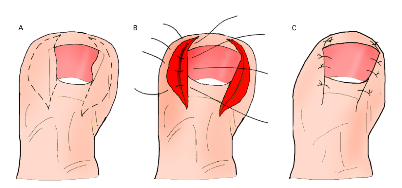
Winograd or Wedge Resection (labiomatrixectomy)
This involves the removal of a wide wedge of tissue including the nail root. This is required when the nail fold is excessive (ungelabia).

Steindler matrixectomy
This is a straight incision to allow the removal of the nail root when the nail fold is normal.
Zadik matrixectomy
This involves removing the entire nail, nail root and matrix. This is needed when the nail has a pincer type deformity, is very peaked or is very thickened.
If there is an infection present this needs to be well controlled before any surgical procedure can be done. Oral antibiotics may be prescribed for you for 1-2 weeks before the surgery.
Plantar Warts
Curettage is usually recommended as a last resort when topical chemical treatment or dry ice treatment has failed. This procedure is also used when a wart is extremely painful to treat.
The operation involves cutting around the wart to include the normal skin margin. The incision is through the full thickness of the skin but no deeper. The surgeon will avoid cutting into the next layer called the dermis, as this is more likely to cause scarring.
A curette is then used to loosen underneath the wart so it can be scooped out as one piece. Phenol (mild acid) is then applied on the dermis where the wart was sitting to ‘mop up’ any viral particles remaining. The tissue can also be destroyed by applying heat generated by the electric current (electrodessication). A crater will be left this area, but it will slowly fill in over the next 4-5 weeks.
Ganglion Cysts
When other treatment options fail or are not appropriate, the cyst may need to be surgically removed. The procedure does require a deep incision often down to the joint or tendon to remove the ganglion where it originates. If it involves the joint spurs in the area may also need to be removed.
Morton’s Neuroma
The operation of choice involves removing the enlarged nerve by a cut made on the top of the foot. The deep transverse metatarsal ligament suspected of causing some of the constriction above the nerve is released. The thickened nerve is then isolated from the surrounding tissue and cut where the nerve trunk appears normal again. An inflamed intermetatarsal bursa is often present and this is also removed. The specimen is sent for a pathology examination.
Hallux Abducto Valgus Deformity (Bunions)
The operation involves removing the enlarged portion of bone. Ligaments and tendons that are too tight around the joint are released. The metatarsal bone in the big toe is then cut and shifted to a normal alignment that also makes the forefoot narrower. The cut bone is held in place with a screw or wire, which is not removed unless it causes problems. The loose, stretched out joint capsule is then tightened completing the soft tissue balance required for your deformity. Both feet can be operated on at the same time, but this does further limit mobility after surgery.
Hammertoes, Mallet Toes & Claw Toes
A common surgical procedure performed to correct a hammertoe is called an arthroplasty. In this procedure, the surgeon removes a small section of the bone from the affected joint. If the contracture is severe it will require additional release of the joint capsule and tendon further up the front of the foot requiring a longer incision. Digital arthroplasty is always performed for a fifth hammertoe deformity to allow flexibility.
Correcting a hammertoe deformity is becoming increasing more common using minimal incision approach. This often involves releasing the tight tendons and making a cut through one or more bones of the toe using a bone cutting burr.
No screws or wires are required for these procedures.